The purpose of a surgical knot is to tie together two fishing lines of different thicknesses (diameters). However, experienced and avid fishermen do not recommend tying a surgical knot on thick fishing lines and undergrowth if the load on the fishing line exceeds 27 kilograms.
The surgical knot is one of the simplest and most durable fishing knots.
This unit is suitable for the main types of fishing lines:
- braids;
- fluorcarbon fishing line;
- monofilament.
How to fix the thread at the base of a surgical suture
Of course, this has an indirect relation to fishing. However, in order to tie a swivel at the end of a fishing line, and for other purposes, it is quite suitable. A description will be given of how to make a fixation using your hands. Experienced surgeons do everything using available tools - clamps, tweezers. This is one of the main advantages of such a knot - the ability to make it using a tool, but more on that later. The use of the instrument saves the surgeon’s fingers from pricks, which saves the doctor from infections when performing operations on patients, for example, HIV or tuberculosis, as well as minimizing contact with large surfaces such as gloves to reduce the likelihood of microbes from outside being introduced into the treated wound.
- At the beginning of the suture, the surgeon threads the needle through the edges of the wound.
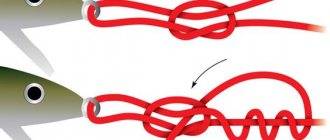
- He then makes a loop, which he crosses on his finger, placing one end of the thread over the other.
- After this, one end of the thread is passed through the loop several times.
- A loop is formed, and it tightens, tightening the edges of the wound.
- Then make another loop on top, passing one end of the thread into it and tightening it. It secures the knot from unraveling quite reliably.
Victoria Leshchenko
I've been working hard in the fishing tackle department for the past six years. I can help you assemble almost any gear.
Ask a Question
This type of knot is used by all surgeons, without exception, at least once in their practice.
results
The average duration of the operation in the studied groups was 72.5±14.7 (Me - 70) minutes for the 1st group with the traditional method of suturing the surgical wound and 65.25±11.9 (Me - 60) minutes for the 2nd group , in which threads with notches were used (Fig. 3).
Rice.
3. Distribution of the duration of surgical intervention in the studied groups (in minutes) (p=0.004). The operation in group 2 was significantly faster than in group 1 ( p
= 0.004).
At the same time, the average wound suturing time for group 1 was 21 minutes, and for group 2, in which barbed threads were used, it was 15.75 minutes (Fig. 4).
Rice. 4. Duration of suturing the surgical wound (in minutes) (p<0.05).
Statistical assessment of intraoperative blood loss indicators in the studied groups was not performed due to zero values, but an analysis of latent blood loss was performed based on the dynamics of hematocrit indicators. The calculation of circulating blood volume was performed according to the method of Nadler et al.: circulating blood volume = K · height (m) 3 + K2 · weight (kg) + K3, where K1=0.3669, K2=0.03219, K3=0.6041 - for men; K1=0.3561, K2=0.03308, K3=0.1833 - for women. In this case, latent blood loss = circulating blood volume (hematocrit before surgery) - hematocrit after surgery [12, 13]. We did not identify any statistically significant differences in the level of hidden blood loss; for the 1st group it was 0.41±0.18 (Me - 0.38) l, for the 2nd group - 0.4±0.18 (Me - 0.38) l ( r
=0.72) (Fig. 5).
Rice.
5. Hidden blood loss (in l) (p=0.72). Blood parameters such as the level of hemoglobin, erythrocytes and hematocrit did not differ statistically significantly in patients of the studied groups before surgery and in the postoperative period (Fig. 6−8).
Rice. 6. Indicators of hemoglobin level before surgery and on the 7th day of the postoperative period in the studied groups (g/l) (p>0.05).
Rice. 7. Indicators of the level of red blood cells before surgery and on the 7th day of the postoperative period in the studied groups (·1012).
Rice. 8. Indicators of hematocrit level before surgery and on the 7th day of the postoperative period in the studied groups.
When assessing the rate of restoration of knee joint function according to the KSS scale and the intensity of pain in the postoperative period, the ability to master the weight of the limb, no significant statistical differences were found in patients of both groups ( p
>0,05).
Over the course of three months after surgery, not a single case of deep periprosthetic infection or thrombosis of the veins of the lower extremities was recorded among patients of both groups. One of the patients developed thromboembolism of small branches of the pulmonary artery during hospitalization with a favorable clinical outcome.
Postoperative complications registered in patients of the studied groups are presented graphically in the table.
For patients with recurrent synovitis included in the study, we considered it necessary to perform puncture of the knee joint on an outpatient basis more than twice, more than two weeks after the operation. In seven patients (4 in group 1, 3 in group 2), after healing of the skin wound and removal of the skin sutures, local marginal skin necrosis or failure of the skin sutures for 1-2 cm was recorded, requiring continued dressing; In these patients, epithelization of part of the skin wound occurred by secondary intention.
Limitations of the study
Of course, our study has limitations associated with the small number of patients examined and the number of patients studied in the groups not being identical. Although modern methods of medical statistics make it possible to determine existing relationships and dependencies with a high degree of reliability.
Our study did not include patients with gonarthrosis accompanied by severe destruction of the knee joint, extreme degree of frontal deformity at the level of the knee joint, or patients with revision knee arthroplasty. In these cases, due to the longer duration of the surgical intervention and, often, significant technical difficulties, the operation time exceeds the permissible exposure time of the tourniquet, and it may be necessary to drain the knee joint, which would violate the conditions of the study.
Using the tool
It's quite simple. In the above example, the needle work is carried out only with the help of a clamp and tweezers.
- The needle is threaded at the beginning of the suture through the wound with tweezers.
- The thread is pulled almost to the end so that a small tip remains.
- It is taken with a clamp, and with tweezers with a needle, the rest of the thread is wound around the end of the clamp four times.
- After this, the tip is pulled through the winding, pulling it off the clamp. It turns out what was in the first example.
- The knot is pre-tightened
- Then they make another loop, dragging the tip with the needle under the tail and tightening it.
This knot is made by professionals in a couple of seconds. After all, time during surgery is of great importance.
Ways of education
Sutures can be applied manually and instrumentally (apodal) method. The predominant knitting method is the hand method. The instrumental approach is used in specific cases, such as deep wounds of complex shape, microsurgery, and endovideosurgery. With the apodal method, the consumption of suture material is reduced. Depending on the number of loops made, the knots can be:
- single-loop,
- two-loop,
- multi-loop.
A knot formed by one loop is used for short-term tissue fixation. In the future, the thread is easily removed after completing the task. Two-loop knots are the most widely used. In medical practice they are used for simple, marine and complex units.
Fishing
One of the main advantages of the surgical unit is that it can work without the use of fingers, but with the help of a tool. All anglers know how difficult it can sometimes be to tie a knot, loop or rig on a line. The cord is very thin and soft. It is difficult to hold it in your fingers, it is difficult to insert the tip into a loop, it is difficult to twist. The cut end may start to get a little frizzy, which makes working with it even more difficult.
Many people completely abandon knots and classic rigs using a cord, and replace them with knotless American ones, as in jig fishing. But a real feeder adheres to traditions and uses a tool - a looper. The looper allows you to make a surgical knot, while making a slightly modified loop, almost like in the previous example.
The difference from the classic surgical knot is the greater strength of the knot made using looper. The fact is that in this case the number of fixing turns of the thread is exactly the same as the main turn. This slightly modifies the surgical knot, allowing you to make non-tightening loops. Working with looper is quite simple; on average, it takes a person a couple of hours to master it. But then you can knit the loops at the same speed as an experienced surgeon fixes the thread at the base of the suture. The Gardner loop is a feeder installation that actively uses the surgical knot.
In addition, you can use a surgical knot for auxiliary purposes. For example, tie the boat that was used to travel to the fishing spot, or tie the awning to the posts. The number of cases when an angler needs a good knot is large. And knowledge of a surgical site will never be superfluous.
Material and methods
302 patients with end-stage deforming arthrosis of the knee joint, tolerant to conservative treatment, requiring total knee replacement, without restrictions on body weight and body mass index, were randomly divided into two prospective groups, differing in the type of surgical wound suturing technique used.
All patients underwent spinal anesthesia using bupivacaine, and 1.5 g of tranexamic acid was administered intravenously 30 minutes before surgery. The operation was performed with the patient in the supine position, with the operated lower limb fixed with an orthopedic table holder; a pneumatic tourniquet was applied to the upper third of the thigh through a tissue lining, which was activated in the position of maximum flexion in the knee joint, creating a pressure in the cuff of 270-300 mm Hg. In all patients, we used an anterior approach to the knee joint (anteromedial - for patients with varus deformity and anterolateral according to Keblish - for “valgus knee”). Using a standard set of instruments, the necessary elements of the soft tissue release were produced, the beds for the endoprosthesis components were prepared, and their cementation was performed. Drainage of the knee joint cavity was not performed in patients of the studied groups.
In the patients of the study groups, the methods of suturing the surgical wound differed:
1st group ( n
=102) in the position of flexion of the knee joint at an acute angle, the joint capsule was sutured with a continuous entwining suture using a braided thread Vicryl 2 (one or two threads with a needle) (Ethicon "Johnson & Johnson"), the subcutaneous fatty tissue was sutured with a continuous entwining suture using a Vicryl 2/0 thread (one - two threads with a needle) (Ethicon “Johnson & Johnson”), the skin was sutured with non-absorbable removable polycaproamide monofilament thread using a continuous suture according to Donati;
2nd group ( n
=200) in the position of flexion of the knee joint at an acute angle, the joint capsule and subcutaneous fatty tissue were sutured with a continuous entwining suture using a bidirectional thread with notches for a continuous knotless Stratafix suture (one thread with two needles) (Ethicon “Johnson & Johnson”), the skin was sutured with a non-absorbable removable polycaproamide monofilament using a continuous Donati suture.
The average age of patients in group 1 was 63.1±7.7 years (Me - 64), in group 2 - 63.09±9.6 years (Me - 64). No statistically significant differences in age values were obtained ( p
=0.9) (Fig. 1).
Rice.
1. Distribution of patients by age. 1st group - traditional threads, 2nd group - threads with notches for a continuous knotless suture (p=0.9). Patients are statistically significant ( p
>0.05) were randomized by gender, women predominated in both groups (82.7% in group 1 and 82% in group 2) (Fig. 2).
Rice.
2. Distribution of patients by gender. A comparison between the two groups was carried out according to the following parameters: volume of intra- and postoperative blood loss (occult blood loss), duration of the operation, duration of suturing of the surgical wound, laboratory blood parameters (hemoglobin, red blood cell count, hematocrit), severity of pain on the VAS scale, recovery rate functions of the knee joint (supportability, amplitude and control of the weight of the limb), the number of postoperative complications.
After receiving baseline patient data, spreadsheets were compiled
Postoperative complications recorded in patients of the studied groups during the observation period using the Microsoft Excel computer program. To statistically process the obtained data, we used the Past ver.3.17 program (2017). To process the data under study, we used nonparametric statistics methods. Samples were compared using the Wilcoxon-Mann-Whitney test or the Kolmogorov-Smirnov test. When comparing dependent samples for the same group of patients, we used the nonparametric Wilcoxon test. To look for correlations between samples, we used the Pearson linear correlation test.
Why loops?
It's simple - loops are the most popular element in feeder installation. With their help, making a Herculean hitch, you can link two fishing lines together, fixing the leash on the main cord. Using the hinges, you can easily install the feeder, and then easily remove it and replace it with another one. Simply by tying the feeder to the fishing line we will get a permanent connection. Almost all installations are made using hinges, or can be made using them.
Another advantage of loops made with loop knitting is that they turn out to be quite small, small in size, and identical. This is very important when making a loop for attaching a leash. When making a loop, the tail turns out to be small, which would be impossible if we were making a loop with our hands, where we would have to enlarge the tip to grasp it with our fingers. If it is done by a good fisherman, then there is no need to cut anything - the fishing line is used very sparingly.
Other fishing devices
The surgical knot is not the only one used in feeder fishing. In addition to the usual looper, there are many other devices for tying other knots. For example, there are crocheters - devices with which you can very conveniently and quickly tie a hook. For those who do not prepare leashes in advance, it will be very useful, because it will allow you to quickly and accurately change the length of the leash.
Another device is a knotter for a shock leader. To tie it, you can use a special device that fixes the shock leader to the main fishing line quickly and without errors leading to the knot untying.
Any angler will appreciate this. After all, they fish with a feeder not only during the day, but also at night, when you have to tie knots almost by touch. And even in the cold wind, when your fingers are numb. The use of devices for tying knots provides comfort, reliability and allows you to spend less time on making equipment and more on the fishing itself. They cost pennies, but bring a lot of benefits.